The HIV Structured Transition EmPowerment (STEP) Program is a multidisciplinary intra-campus health care transition program to support youth with HIV as they transition from pediatric to adult HIV care. In 2017, the University of Maryland developed and launched STEP, an integrated health care transition program where the adult HIV clinical team is assimilated into the pediatric/adolescent clinic and collaboratively transitions young patients to adult care using individualized transition plans. Ninety-five percent of youth enrolled in STEP were still retained in adult care at 12 months compared to only 50% of a pre-STEP cohort.
Baltimore, MD

Health care transition, defined as the purposeful planned move of youth with special health care needs from pediatric- to adult-centered health care, can be a vulnerable time for youth with HIV. Multiple barriers to transition include poor communication between pediatric and adult HIV care, differing philosophies of care, young people not wanting to leave their trusted pediatric providers, and the need to transition to other services (e.g., behavioral health, support services) in addition to HIV health care. While there are no evidence-based strategies for successful HIV health care transition for youth moving from pediatric to adult HIV care, some best practices have been identified that support these changes in care. These include a multidisciplinary health care transition approach (including wrap-around services), early and integrated involvement of an adult care team, optimal communication between pediatric and adult care teams, and individualization of the health care transition plan.1,2
The health care transition clinic is embedded in the Pediatric/Adolescent HIV clinic but staffed by an adult HIV health care provider and health care transition navigator.
Prior to enrollment in the STEP Program, patients receive education regarding broad concepts of health care transition starting at age 13. Starting at age 18, youth are oriented to the STEP program, and may informally meet at least annually with the STEP provider and/or health care transition navigator. During this time, their care is still provided in the Pediatric/Adolescent HIV clinic and overseen by pediatric/adolescent providers.
Patients can enroll in the STEP health care transition clinic after age 20; while there is not a fixed age to transfer to adult HIV care, the suggested age is around 24. While enrolled in the STEP clinic, these individuals primarily interact with the adult HIV provider, health care transition navigator, and pediatric social worker and pediatric case manager; the STEP adult team members (specifically social worker and case manager) may attend these visits to foster a durable relationship with the person post-transition. Patients are assessed for transition readiness and an individualized transition plan is collaboratively developed by the STEP team and the patient.
During the transition period, the patient, with support from the STEP team, schedules and attends their first adult clinic visit. This transfer to adult care involves pediatric and adult STEP team preparation, and adult STEP team involvement at this linkage to adult care visit. Transition to the adult HIV clinic is considered official after the completion of this linkage visit.
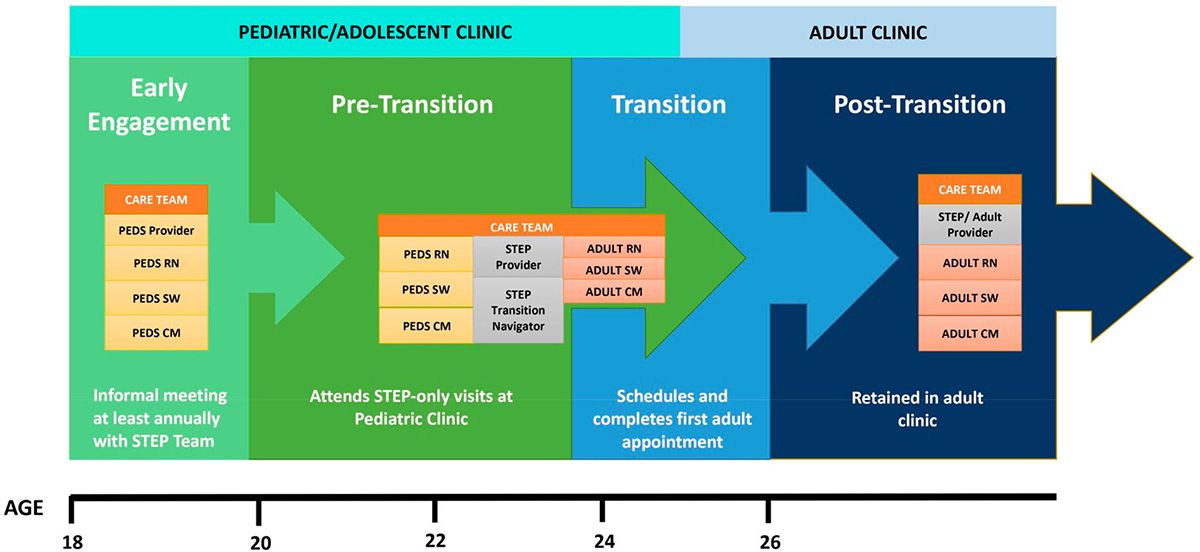
All youth enrolled in the STEP Program at any stage of transition are followed closely though a retention database. The STEP team meets monthly to assess retention in care for STEP participants, including those who have completed transition to adult care. When retention concerns arise, the team will strategize to address barriers to retention and ensure the young person remains in care.
Thirty-four youth were enrolled in STEP from July 2017 to January 2020 and followed for 12 months or until they had two adult clinic visits. Successful linkage to adult care occurred in 32 of 34 patients (94%). Compared to a pre-STEP cohort, (n=50), STEP participants were nearly twice as likely to be retained in adult HIV care at 12 months.
| Category | Information |
|---|---|
| Evaluation data |
|
| Measures |
|
| Results |
* statistically significant |
Source: Ryscavage P, Herbert L, Roberts B, et al. Stepping up: retention in HIV care within an integrated health care transition program. AIDS Care. 2022;34(5):554-558.
GOT Transition Program framework. The STEP Program is built upon principles outlined in the GOT Transition Program3 and includes six key components of the care transition process: developing a transition policy or guide and sharing it with patients and providers; tracking and monitoring; assessing transition readiness; developing an individualized health care transition plan; transferring of care; and confirming the transfer.
Development of transition policy and a database for data sharing. The STEP team created a transition program policy and protocol which is available for all youth transitioning and providers. They also facilitated data sharing between pediatric and adult providers by maintaining a database that tracks pre- and post- transition retention information.
- Adult care team integration into the pediatric clinic involves not only the onsite presence of an adult HIV provider and health care transition navigator, but also collaboration with adult case management and social work while the young person is still in pediatric care. This integration is essential given the challenges facing youth undergoing health care transition, including the need for transition of concurrent behavioral health services and/or other case management needs such as housing or transportation.
- While retention in adult HIV care at 12 months was high, it will be important to follow longer term retention in care beyond this time frame given concern for “clinic burnout” among young adults. This is highlighted by the considerable work by the STEP team which went into maintaining retention despite a 35% no show rate seen in adult care.
- CDC Compendium: Structured HIV Transition EmPowerment (STEP) Program
- Got Transition (Got Transition is the national resource center on health care transition).
- Philbin M, Tanner A, Chambers B, Ma A, Ware S, Lee S, Fortenberry JD, The Adolescent Trials Network. Transitioning HIV-infected adolescents to adult care at 14 clinics across the United States: Using adolescent and adult providers’ insights to create multi-level solutions to address transition barriers. AIDS Care. 2017;29(10), 1227–1234. doi:10.1080/09540121.2017.1338655
- Tepper V, Zaner S, Ryscavage P. (2017). HIV healthcare transition outcomes among youth in North America and Europe: A review. J Int AIDS Soc. 2017; 20(Suppl 3), Article 21490. doi:10.7448/IAS.20.4.21490
- Got Transition. gottransition.org