
Summary
Module on the major steps required to get going in buprenorphine certification and administration.
Materials Needed
- A computer and compatible LCD projector to play the PowerPoint presentation.
Slide #22: DATA 2000
- The Drug Addiction Treatment Act of 2000 (DATA 2000)
- This enabled qualifying physicians outside of opioid treatment programs (i.e., methadone clinics) to prescribe and/or dispense Schedule III, IV, and V opioid medications approved by the FDA.
- Buprenorphine, as a Schedule III narcotic, could now be prescribed in office-based settings by qualifying physicians.
- Currently, buprenorphine/naloxone is available as a tablet (Suboxone) or film. Both are made to be dissolved under the tongue. Buprenorphine is also available as a tablet in generic form.
Slide #23: Prescribing Buprenorphine
- Who can prescribe buprenorphine? Physicians with:
- Subspecialty board certification from the American Board of Medical Specialties
- Addiction certification from the American Society of Addiction Medicine
- Subspecialty board certification from the American Osteopathic Association
- Completion of 8 hours of approved training from a certifying board.
- Physicians must submit a waiver and notify SAMHSA of intent to dispense or prescribe opioid treatment.
- Typically, 45 days after submitting waiver request, physicians receive an identification (ID) number and the Drug Enforcement Administration (DEA) registration number (to be included on all prescriptions). For the first year, authorized physicians can treat up to 30 patients. After 1 year, they can submit another request, this time to treat up to 100 patients.
Slide #24: Diagram of the Waiver Process
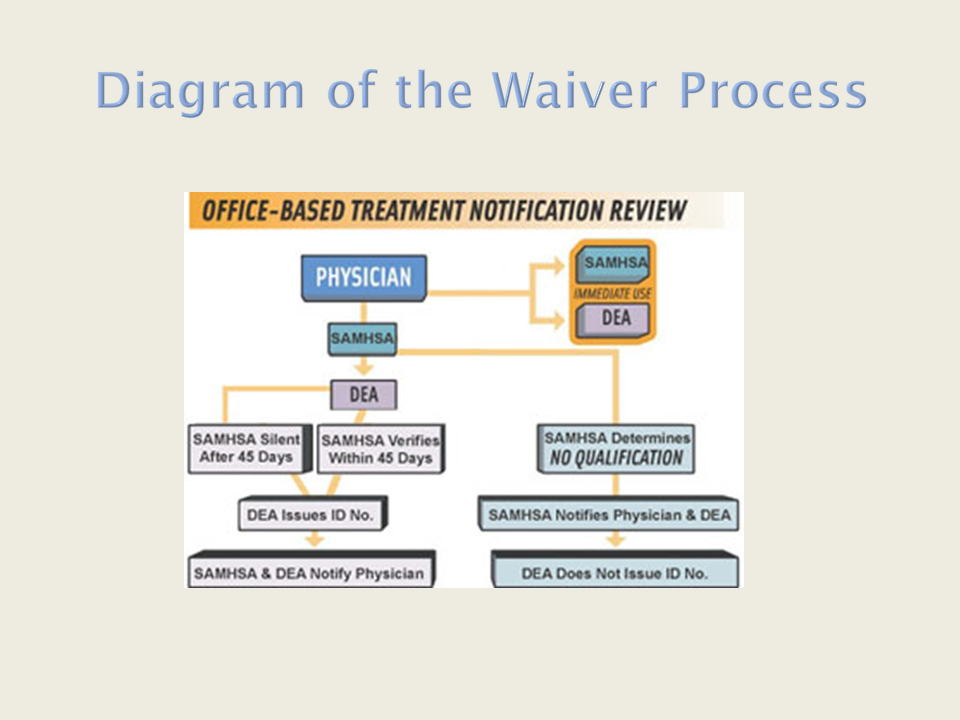
- Here you see a diagram from SAMHSA of the waiver process and its various steps.
Slide #25: Setting the Stage for MAT
- Prepare program- and clinic-wide communication to best facilitate administration of buprenorphine-based MAT.
- Establish and maintain a system to allow clear communication across program staff and volunteers, patients, residential and outpatient addiction treatment and mental health-care providers, and other stakeholders, such as city and State health departments and correctional facilities, so they are aware of policies and procedures.
- Address structural issues: Create appointment slots, assign exam rooms, and add more clinic space if needed.
- Work with pharmacies to ensure and monitor the supply of buprenorphine, and identify resources to help with reimbursement.
- Offer clear, patient-centered buprenorphine education, and describe program expectations.
- Prepare patients for induction. (One program developed "kick packs" with medications to alleviate withdrawal symptoms.)
- Establish and maintain linkages with mental health-care providers in the community to ensure that individual and group counseling is available to patients, both onsite and offsite.
- Facilitate support groups.
- Provide additional resources to all staff for support, mentoring, and training, as well as regular program updates.
- Develop a process for program monitoring and evaluation.
Slide #26: Staffing
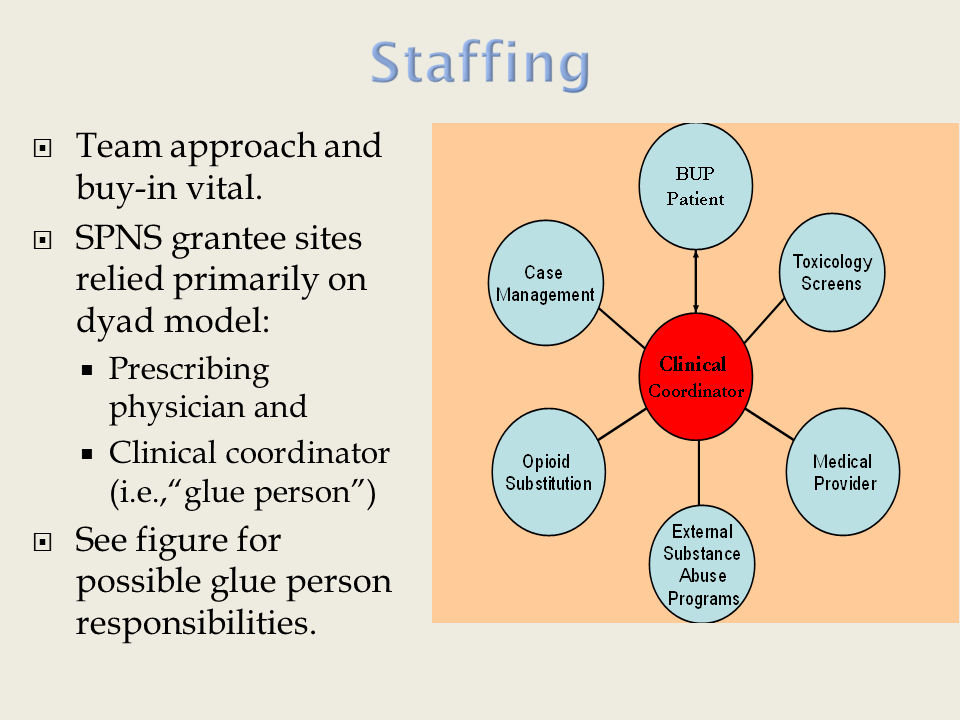
- Although a team approach is key to successful implementation and administration of MAT, SPNS initiative grantees have identified a key staffing configuration: a dyad, involving both a prescribing physician and an accessible service provider, who is often called the "glue person" or buprenorphine coordinator.
- The glue person may be a nurse, pharmacist, or nonclinician who is closely supervised by medical and mental health care providers. The glue person has experience with, and training in, providing services to people with substance use disorders, and receives additional training in addiction medicine, pain management, and other related areas.
- The glue person facilitates implementation of MAT in HIV primary care settings by serving as the point of contact for patients, providers, and issues related to buprenorphine.
- The glue person arranges or provides counseling, case management, outreach, and all other ancillary services.
Slide #27: Three Phases of Buprenorphine Treatment
- The three phases of buprenorphine treatment are induction, maintenance, and stabilization.
- Phases are completed in that order, so no one phase can begin until the previous phase is complete.
Slide #28: Induction
- Induction is the term for buprenorphine initiation, which is done under medical supervision in a doctor’s office. Usually, the first induction visit lasts 2 to 4 hours; the induction phase usually lasts 7 days.
- The goal of induction is to identify the lowest possible buprenorphine dose that will allow patients to reduce or stop their opioid use without experiencing withdrawal symptoms or uncontrollable drug cravings.
- Patients must be in the early stages of withdrawal to undergo induction, because buprenorphine causes acute withdrawal in people who have opioids in their bloodstream. Therefore, use of opioids must be avoided for 12 to 24 hours before induction.
- The Clinical Opioid Withdrawal Scale (COWS) can be used to assess withdrawal symptoms before initiating buprenorphine.
The COWS Scale* is included in the training manual that complements this curriculum.
- If patients are experiencing withdrawal symptoms on day 2 or day 3, buprenorphine dose adjustments may be necessary.
*Note: This publication is a non-Federal resource and is included in order to provide additional information. The views and content in these resources have not been formally approved by the U.S. Department of Health and Human Services (HHS) or the Health Resources and Services Administration (HRSA). Listing these resources is not an endorsement by HHS or HRSA.
Slide #29: Stabilization
- During the stabilization phase, which lasts 1 to 2 months, patients should be seen on a weekly basis in case further dose adjustments are necessary. When people receive the proper dose of buprenorphine, they will not experience withdrawal symptoms or strong drug cravings.
- Usually, people will reduce or stop their drug use during stabilization; if opioid use continues, consider dose adjustment.
Slide #30: Maintenance
- Once patients are medically stable, they may remain on buprenorphine indefinitely; there is no set length of time that patients remain in this phase. The SPNS initiative lasted 5 years.
- Counseling is an important part of maintenance, since people are able to address psychosocial issues.
- If patients wish to discontinue buprenorphine, dosing should be gradually tapered unless there is a reason for patients to stop buprenorphine more rapidly, such as relocation or travel to a country where it is not available, upcoming incarceration, or conditions of employment.