 Session Length: 25 to 35 minutes
Session Length: 25 to 35 minutes
 Time variance accounts for potential guest community clinical expert; see slide #19
Time variance accounts for potential guest community clinical expert; see slide #19
 PDSA Cycle
PDSA Cycle
Summary
This section provides an overview of the continuum of care and guides discussion about:
- Hard-to-reach PLWHA populations the clinic currently serves and/or wants to serve,
- What steps currently are being taken to identify and engage hard-to-reach PLWHA into care, and
- What can be done to improve and ramp up these efforts.
Materials Needed
- Computer and compatible LCD projector to play the PowerPoint presentation
- Notes from Module 1
- Paper and easel
- Colorful markers
- Tape for affixing paper to the wall as necessary
- Copies of the Module 2 handouts to distribute
- Invited guest speaker(s), as needed.
Module 2 features both teaching material and guided group discussion.
The Facilitator or other appointed person should write key thoughts voiced by participants throughout the presentation and subsequent discussions on the paper/easel.
Before beginning the presentation, distribute the Module 2 handouts, Continuum of Care and Common Terms and Definitions.
The handouts start at the end of the section for easy printing/ copying.
The Facilitator introduces the first slide, which refreshes participants about the last session. Participants should review the Continuum of Care Handout as well.
Slide #16: Training Refresher
Before we begin, let’s review the previous session. Namely:
- Why should PLWHA engage in HIV care as early as possible in their infections?
- What populations have been most impacted by HIV and why?
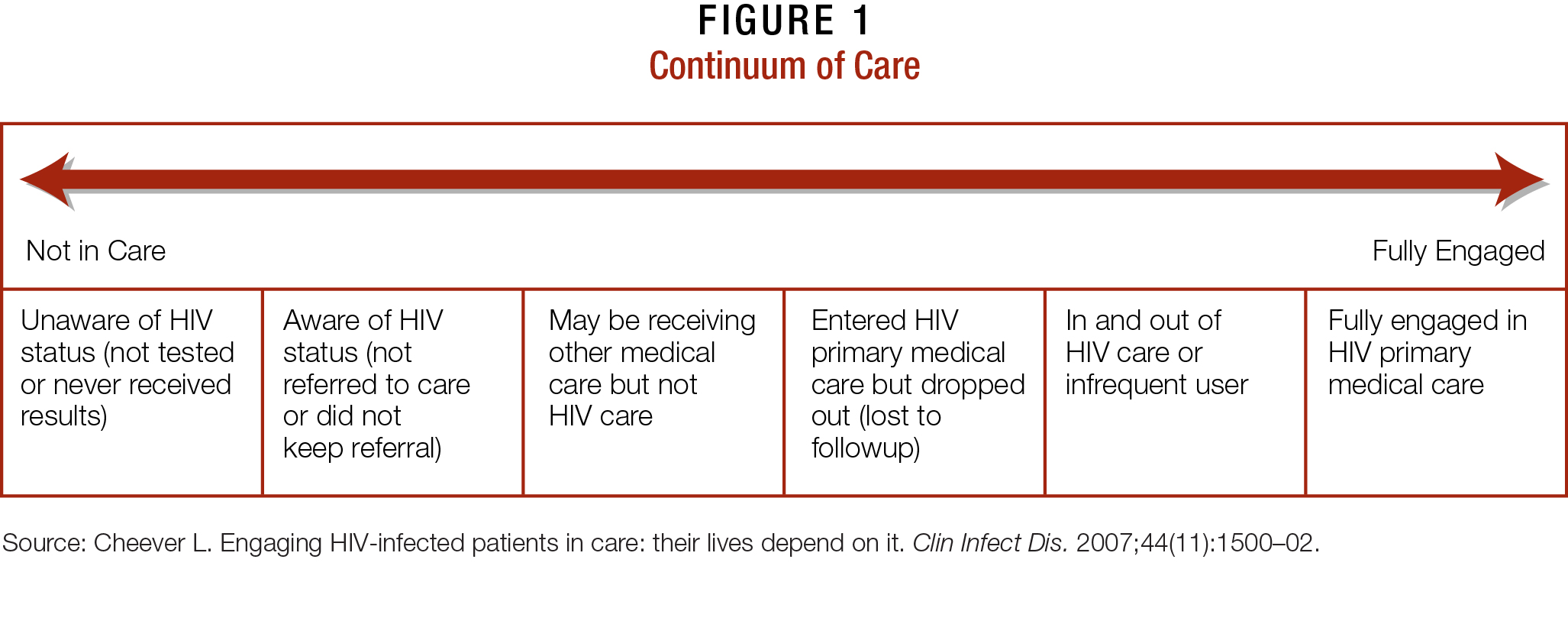
Slide #17: The Continuum of Care
Engaging in HIV care involves a spectrum of activities, not a singular event.
It begins with PLWHA learning their serostatus and ideally reaches the point where they become fully engaged and retained in HIV primary care.
Slide #18: The Continuum of Care: A Spectrum
- A patient’s location on the continuum is not static. PLWHA move up and down the continuum.
- Movement away from full engagement often occurs in response to
unmet needs, including:
– Food insecurity and shelter instability, poverty, SUDs, mental illness, and other psychosocial and economic determinants.
– PLWHA with limited educational attainment and histories of incarceration also have difficulty obtaining and maintaining employment and health insurance, which can further delay them from accessing care.
– It is not uncommon for PLWHA to ignore their health needs until they require emergency room assistance. Seeing an HIV primary care provider may be their first ongoing experience with the health-care system. - Full engagement and retention in care is essential for PLWHA to achieve optimal health outcomes.
– These include engagement in healthy behaviors; reduction in high-risk behaviors; and better overall health.
– Engagement and retention in care supports ART adherence, which suppresses HIV viral loads and improves the health of individual clients, while significantly reducing their chances of transmitting the virus to others.
People with undetectable HIV viral loads are less likely to transmit the virus.
Slide #19: Care and Treatment Adherence Lowers Community Viral Load
The Facilitator may want to bring in a community expert to discuss the community viral load in the local community. If an expert speaks, provide them approximately 10 minutes to do so. They should speak after this slide but before the subsequent group discussion.
- Engaging PLWHA in care and helping them become adherent to ART can improve health outcomes not just for the individual, but for their entire community.
- This can be monitored through a measure called community viral load (CVL).
– ART-adherent PLWHA can achieve significant reductions or undetectable levels of HIV in their bloodstreams. The amount of virus in the bloodstream is determined through a laboratory test, and the resulting measure is referred to as a viral load. It is an essential clinical benchmark for PLWHA.
– Individual viral loads for an entire PLWHA population can be aggregated and averaged, resulting in a CVL. The CVLs of different populations can be compared and disparities identified.
– A community’s CVL can be lowered by engaging its PLWHA population into care and helping them become ART-adherent. A lower CVL also points to fewer HIV infections, since PLWHA with low or undetectable viral loads are less infectious.
How do you think the CVL of the populations we serve compare to one another and why?
Slide #20: Module 2 Activity
The Facilitator now engages the group in a discussion about what was covered in the first module, referencing the notes created. (Ideally, the paper and easel from Module 1 will be easily visible for all participants.)
- Review the vulnerable PLWHA populations currently served by the clinic that participants identified during Module 1.
- Where are most of these populations currently located on the continuum of care?
Slide #21: Module 2 Activity, Continued
The Facilitator goes around the room and asks participants the following questions. Notes should be recorded.
- Are there PLWHA populations the clinic wants to target more effectively?
- What activities currently take place (if any) to recruit, engage, and reengage these populations into care?
- Are these activities informal or formal?
- Are dedicated staff, funding, and other resources set aside for these activities?
- If the clinic serves multiple vulnerable PLWHA populations, discuss whether different strategies are used—or should be used—to recruit, engage, and retain them into care.
The presentation ends with a review of the module’s goals and the remainder of the upcoming modules.
Slide #22: IHIP Process and the PDSA Cycle
The curriculum is designed to help us prioritize, plan, implement, and review these models of care within our operations.
Each module conforms to the PDSA model, shown here. It’s conceived as cyclical and iterative, as necessary.
Slide #23: Replication Steps
- The planning modules will help participants discuss what they want to achieve in implementing one or more of these new model(s) of care.
- The doing modules will guide the work involved in achieving the steps outlined in the planning stage.
- The modules in this curriculum primarily are geared to helping us reach the study (or evaluation) and act (final incorporation and execution) stages of the PDSA cycle.
- However, the doing modules include a Group Evaluation activity, which serves, in part, as the study piece of this curriculum’s PDSA cycle.
Save the notes from this and previous modules for reference in future sessions.
CONTINUUM OF CARE HANDOUT
Common Terms and Definitions Handout
| Term | Definition |
|---|---|
| Adherence to ART | Adherence means taking medication regularly, as prescribed. Antiretroviral Therapy (ART) adherence refers to patients who take their HIV medications as instructed nearly 100 percent of the time. Adherence is essential to preventing drug resistance, significantly lowering or achieving undetectable viral loads, and subsequently improving PLWHA health outcomes and reducing transmission risk. |
| Community Viral Load | The average of all viral loads of a specific community of PLWHA results in a measurement called the “community viral load” (CVL). The CVLs of different populations can be compared and disparities identified and addressed. Lowering a community’s CVL requires PLWHA to become engaged in care and ART-adherent, since this means they are likely to have low or undetectable viral loads and less likely to transmit the virus to others. |
| Engagement in Care | Engagement refers to an ongoing series of interactions between PLWHA and a continuum of care with a variety of providers, including outreach workers, case managers, clinic staff, medical personnel, counselors, ancillary service providers, etc. Clinically, patients are considered engaged in care if they have had at least 1 visit in each 6-month period with a single HIV care provider within a 12-month period. |
| Full Engagement in Care | Full engagement in care occurs when PLWHA have a complete, regular, ongoing involvement in primary medical care. Similar to “engagement in care,” it is clinically defined as 2 visits within a 12-month period that are at least 3 months apart. |
| Health Service Navigator | Health Service Navigators (HSNs) are staff members trained to provide intensive case management for PLWHA entering care and/or may be accessing services from partnering providers. HSNs may conduct care assessments and develop action plans to help their clients identify their care goals and understand how they can reach them. |
| Intensive Case Management | Intensive case management involves coordination of medical, mental health, and other services in the context of frequent meetings and check-ins, often for a set period of time. |
| Linkage to Care | Linkage involves the initial connections and entry points of care after HIV testing and disclosure. Linkage may include referral by a case manager to a treatment program for substance use disorders (SUDs) as well as medical and mental health care. In addition, persons who test negative for HIV may be linked to a peer counselor for additional guidance around HIV prevention. |
| Lost to Care | Patients who have had at least 1 visit in the last 2 years with a provider, but have not been to the facility within the last 12 months. |
| Outreach | Outreach is a series of singular events geared to finding people who are at risk for or living with HIV, to offer education and to link people to HIV testing and care. These events can include health fairs and encounters outside entertainment venues. They generally do not refer to ongoing activities that retain people into care, such as appointment reminders. |
| Peer/Near-Peer | Peers and near-peers are outreach workers or counselors who encourage people at risk for HIV to get tested, and work to keep PLWHA engaged in HIV prevention, care, and treatment. Often peers and near-peers are from the same ethnic and racial background and the same general age as the clients they serve. |
| Retention in Care | Describes ongoing, full engagement of PLWHA in care over time. Sometimes used synonymously with “full engagement in care.” |
| Reengagement | Reengagement refers to patients who return to care after having fallen out of care in the past. |
| Sporadic Care | Clinically, sporadic care refers to patients who have seen an HIV provider no more than 1 time in a 12-month period. These patients would be considered unstable in care. |
| Time-Limited | Time-limited interventions take place during a set time period. For instance, a new, reengaging, or unstable patient may receive intensive case management until he/ she is stable and able to better navigate their care independently. |
| Unstable in Care | Patients who are unstable in care—indicated through factors such as missed appointments, not being adherent to ART, and SUDs—are considered at risk and on the verge of falling out of care. |