60 minutes
This can be broken down into two 30-minute sessions if necessary. (First session will include slides #25 to 31, including associated discussion questions within those slides. Second session will include slides #32 and #33 as well as the “Outreach: Role Play” activity.)
PLAN module
Summary

To better engage current or new vulnerable PLWHA populations, clinics are encouraged to replicate one or more of the models of care described in this curriculum.
This module provides a brief overview of the models of care developed through the SPNS Program. Particular emphasis is placed on the traditional street/social outreach model of care.
Participants will discuss the pros and cons of this model of care in targeting the marginalized and underserved PLWHA they wish to serve.
Materials Needed
- Computer and compatible LCD projector to play the PowerPoint presentation
- Notes created during previous modules
- Paper and easel(s)
- Colorful markers
- Tape for affixing paper to the wall as necessary
- Copies of the Module 3 handouts to distribute
Module 3 features teaching material, guided group discussion, and a group activity.
The Facilitator or other appointed person should write key thoughts voiced by participants throughout the presentation and subsequent discussions on the paper and easel.
Before beginning the presentation, distribute the Module 3 handouts: Models of Care, Traditional Street/Social Outreach Logic Model, Outreach Encounter Form, and Model of Care Evaluation.
The handouts start at the end of the section for easy printing/copying.
The Facilitator should introduce the first slide, which serves as a refresher about the last session. It may be helpful to have notes from previous module up for display to foster discussion.
Slide #25: Training Refresher
Before we begin, let’s review the last session.
- What PLWHA population(s) do we want to engage more effectively?
- Where are the PLWHA populations we serve (and wish to serve) on the continuum of care?
Slide #26: Innovative Models of Care
Through this course, we are going to review several different innovative models of care geared to helping clinics like ours engage in care.
The Models of Engagement being outlined include:
- Traditional Outreach/Social Outreach Model
- Motivational Interviewing Model
- Health System Navigation/Retention in Care Coordination
- HIV Interventions in Jails
- In-reach (reconnecting with past patients lost to care)
- Social Marketing Campaigns/Social Networking Channels.
Slide #27: Traditional Street/Social Outreach
Traditional Street/Social Outreach is perhaps the best-known model of care in the HIV/AIDS arena. It generally involves:
- Brief, singular encounters with persons in areas where targeted PLWHA live, work, and otherwise frequent, including public areas and events.
- Most often staffed by peers or near-peers of the target population(s). They tend to be trained volunteers or entry-level staff. They may be “stationed” in designated areas in a group or at a booth/table. They also may use the clinic health van as a central location.
- Giveaways, such as condoms, bleach kits, and brochures, are often distributed. Oral swab HIV testing, when available and allowed, is also offered (sometimes under the guise of general health services) to avoid HIV stigma.
Who would like to share their experiences conducting outreach work? Tell us about:
- Your target audiences/populations.
- The type of outreach activities you conducted, noting what worked and didn’t work.
Slide #28: Traditional Street/Social Outreach: A Breakdown
Let’s discuss the pros and cons of this model of care. First, the pros:
- It offers an effective tool to reach nearly all populations, particularly when used in a health van setting. In those instances, general health services can be provided along with HIV testing, offering potential patients a greater sense of confidentiality.
- An official case manager can be stationed onsite to offer those who test positive onsite referrals and/or a chaperoned escort to the clinic for continued testing and linkage to treatment and care.
And then the cons:
- Outreach workers tend to turnover pretty quickly—particularly when they are younger and/or volunteers. That means having to train more often.
- These encounters are often singular in nature. People who get tested through outreach activities tend to be members of highly mobile populations, and their contact information can change frequently; they can easily be “lost” to the clinic if they fail to follow up on a referral.
- We may need to get solicitation licenses and register to appear at exhibit halls.
- Health van purchase, licensing, and maintenance can be costly.
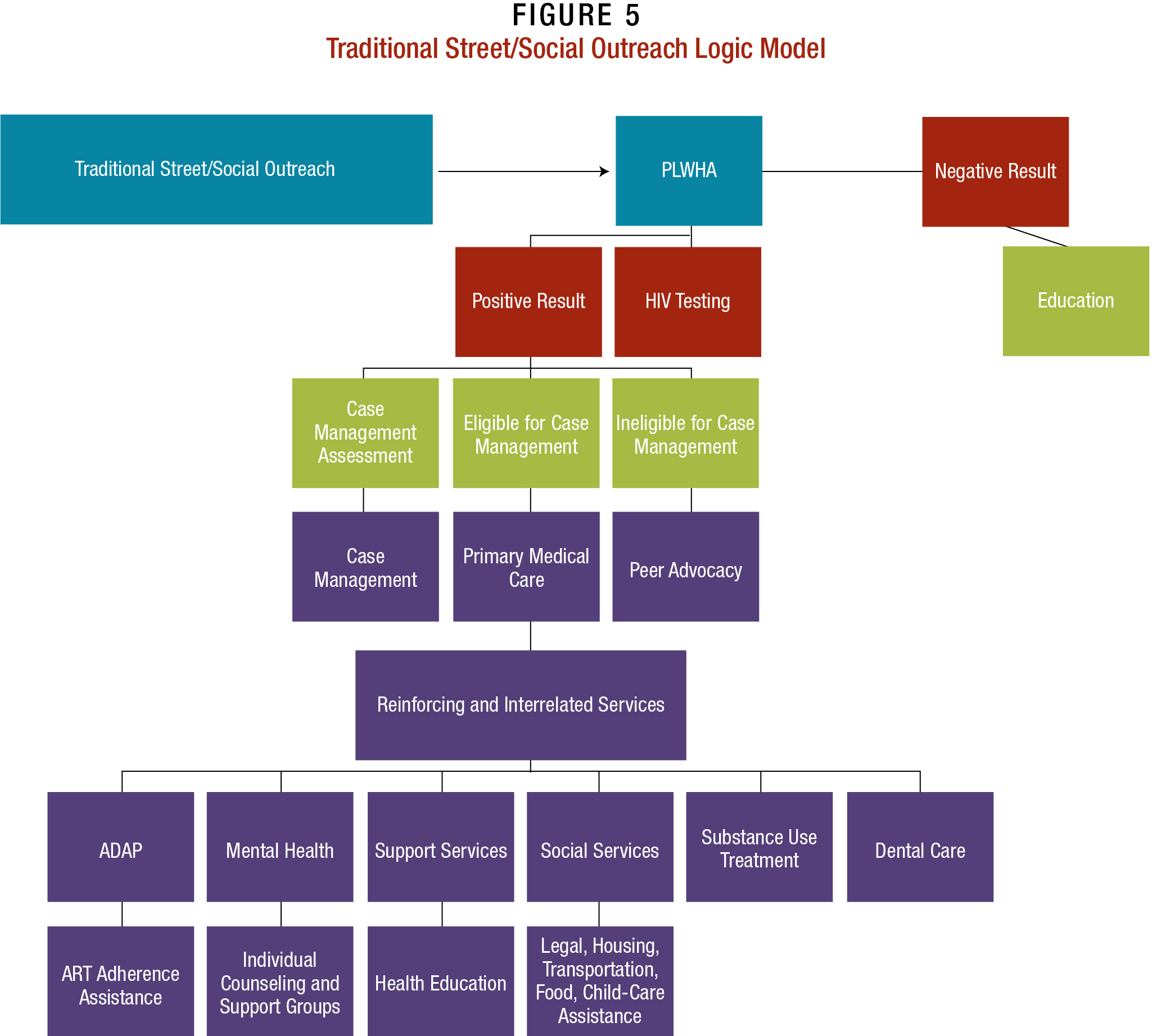
Slide #29: Traditional Street/Social Outreach Logic Model
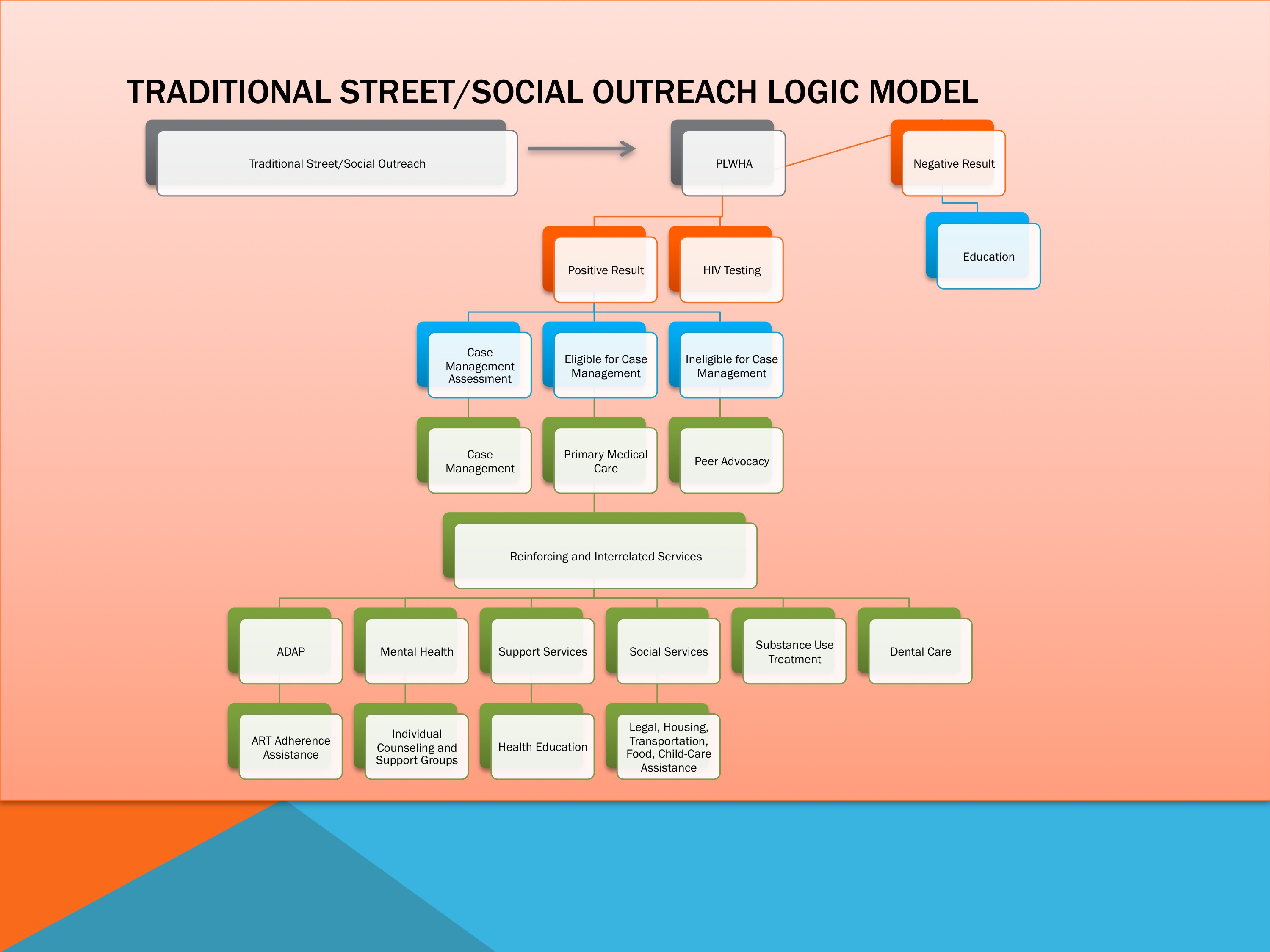
Here we have the traditional street/social outreach logic model.
We follow a patient from an initial encounter to engagement in care.
Slide #30: Traditional Street/Social Outreach Logic Model, Continued
The logic model offers an idealized vision of outreach.
What do you think of this model of care? Do you think it describes how it might work at our clinic?
Slide #31: Traditional Street/Social Outreach Logic Model, Continued
 There are logistical issues to consider with this model of care, which could lead to increased costs.
There are logistical issues to consider with this model of care, which could lead to increased costs.
First issue up: staffing.
- We all need to be on board with this approach, or it isn’t going to work. We are doing this training, but what about focus groups? Other forms/methods of achieving buy-in?
- Should we bring consumer voices from the clinic, the local Ryan White Planning Council, and other entities into this process?
- Outreach workers represent us to the public. Should we have both experienced and new staff onsite to bring PLWHA into the clinic?
- Does the clinic have personnel already trained or who can be easily trained to serve as outreach workers for the clinic? Will staff need to be hired?
- What types of training do you think outreach workers need?
- If we offer onsite oral swab HIV testing, what will we do about providing specialized training? Also, should we have a case manager onsite to work with those who have a reactive test?
Second up: Protocol or the official way we set up our outreach.
- How will the agency present itself during outreach? Will staff wear anything that connects them with the clinic, such as t-shirts or backpacks? Or will they be anonymous in an attempt to enhance patients’ sense of confidentiality?
- How will encounters be conducted? Will outreach workers use a script/form to guide their conversation and capture data? (See the Outreach Encounter Form Handout.)
- Will the clinic be able to leverage notebook computing, data-tracking software, and wireless Internet connectivity to track interactions? Who will be responsible for data collection during and after outreach encounters?
- What about confidentiality? How do we safeguard the identity of the people we contact?
Venues and Materials: The clinic also will need to consider questions such as:
- Do we know where to find our target populations in the field? Where will we go? Clubs? Public transportation areas? Health fairs? Cultural events?
- If we don’t find our target population, are we willing to work with other PLWHA?
- Will we hand out materials to those we meet? Will the materials be branded with our clinic name or logo, or be generic? What will we hand out? Condoms, harm-reduction materials (as allowed) and/or educational materials?
- We may need to talk again about getting solicitation permits, as well as the rental, licensing, and maintenance of a health van or other vehicle.
Slide #32: Module 3 Group Activities
Please refer to the Group Activity description below.
We are now going to play two different games. The first is “Outreach Hot Seat.”
I’m going to select someone to play the “outreach worker” assigned to approach potential clients at a local nightclub. You are going to answer, in character, the following questions:
- Are you working inside or outside the club? Both?
- Does the nightclub know you are recruiting possible PLWHA? Did the nightclub help promote these outreach efforts? Did the clinic? Are you working together? Perhaps you are not promoting your outreach work at all? Is this a set ongoing outreach event at this venue?
- Are you wearing clothing or handing out materials branded with the clinic’s name?
- Are you handing out giveaways? If so, what are they?
- How do you approach potential patients? Do you have an outreach form or memorized script to guide the conversation?
- What do you do when turned down by the person you approach?
- What do you do when they say yes?
- Are you offering general information, overall health care, giveaways, HIV testing?
- How are you ensuring patient privacy? Where are you speaking with potential patients? In a health van? In the venue itself?
- Are you providing pre- and post-HIV testing counseling?
- Are you working alone or with someone? If there is HIV testing, how are you dealing with those who have a reactive test? Are you linking/referring them to care? Driving them to the clinic?
- What about those with a nonreactive test? Do you provide them additional information? Counseling? Referrals to other services, such as shelters, and clothing and food banks, as necessary?
- During and after the encounter, how do you handle the data you capture?
- What other issues might arise?
The second game is “Outreach Role Play.”
I’m going to select two volunteers—one to play an outreach worker and the other a potential patient—to act out the following scenarios:
- An ideal outreach encounter that goes just as the clinic would want.
- An outreach encounter that does not go as planned. For example:
– The potential patient is not interested in being approached or voices concerns about confidentiality.
– You meet someone who is interested in getting tested, but is
not exactly a member of your target PLWHA population(s).
– You engage a patient who has a reactive HIV test, but does
not want to be referred to services.
Lead the discussion on whether this model of care will work for the clinic. Have participants refer to the Model of Care Evaluation Handout from Module 3.
Tape several pieces of paper with the model of care’s name on each.
Slide #33: Group MODULE Evaluation
Read each question and then write down everyone’s thoughts, questions, suggestions, etc. on the paper.
- Can this model of care be readily integrated within the clinic’s current operations and help it reach targeted populations of PLWHA?
- Does the clinic already use this model of care, perhaps in a slightly different form?
- Can the clinic satisfy all requirements for this model of care?
- What funding streams, staffing, materials, and other resources are necessary to implement this model of care? Does the clinic have access to these? If not, how will they access them?
- How will buy-in be secured within the clinic?
- Will the implemented model of care be promoted to potential patients? If so, how? Online through social networks? Word of mouth?
- Does this model of care help the clinic identify and engage targeted PLWHA populations into care?
- Compare the pros and cons of this initiative.
If more than 10 people are present, the Facilitator may split participants into two or three groups to discuss the following questions and write their thoughts on the paper. After a few minutes, the Facilitator can reconvene everyone and have a representative from each group explain everyone’s ideas.
Save the paper from this and previous modules for reference in future sessions.
| Models of Care | Definition |
|---|---|
| Traditional Street/Social Outreach Model | This outreach model often involves having peers engage in outreach with at-risk persons in their communities, often in public arenas, such as public events and entertainment venues. |
| Motivational Interviewing Model | Rather than a singular outreach event, motivational interviewing (MI) is delivered by peers and near-peers, who are trained to provide culturally and linguistically competent counseling. MI is designed to help patients align their behaviors with their treatment goals so they become engaged and retained in care. |
| Health System Navigation/ Retention in Care Coordination | HSNs work with PLWHA clients to support engagement in care with partnering providers. They conduct assessments, codevelop action plans with PLWHA, and coordinate care across providers. |
| HIV Interventions in Jails | This model leverages the jail setting (and related correctional institutions such as parole offices) to identify and engage PLWHA into care. The uniqueness of HIV care in jail settings involves its own model, which in part is a hybrid of several others in this training manual. |
| In-reach (reconnecting past patients lost to care) | Providers work with partnering agencies and use their databases as a resource to identify PLWHA who have fallen out of care, contact them, and help them to reengage in care. |
| Social Marketing Campaigns/ Social Networking Channels | Social marketing uses commercial advertising techniques to “sell” HIV prevention, testing, treatment, and care through messages targeted to specific populations. Television and radio advertisements and promotional materials are often repurposed and circulated online through social networks, such as YouTube, Facebook, and Twitter. |
Traditional Street/Social Outreach Logic Model