 Session Length: 30 minutes
Session Length: 30 minutes
 PDSA Cycle
PDSA Cycle
Summary
This module provides an overview of the health system navigation/ retention in care model of care. Participants will discuss the pros and cons of this model of care in targeting the marginalized and underserved PLWHA they wish to serve.
Materials Needed
- Computer and compatible LCD projector to play the PowerPoint
presentation - Notes created during previous modules
- Paper and easel(s)
- Colorful markers
- Tape for affixing paper to the wall as necessary
- Copies of the Module 4 handout to distribute
- Invited guest speaker(s), as needed.
Module 4 features teaching material, guided group discussion, and a group activity.
The Facilitator or other appointed person should write key thoughts voiced by participants throughout the presentation and subsequent discussions down on paper.
Before beginning the presentation, distribute the Module 4 handout, Health System Navigation/Retention in Care Coordination Logic Model.
The handout starts at the end of the section for easy printing/ copying.
The Facilitator should introduce the first slide, which serves as a refresher about the last session. It may be helpful to refer to notes from previous sessions to jumpstart discussion.
Slide #35: Training Refresher
Before we begin, let’s review what we thought were the pros and cons of the previous model we reviewed.
Slide #36: Health System In-Care Navigation/Retention in Care Coordination Logic Model
Health System Navigators (HSNs) help PLWHA access HIV/ AIDS care services from different providers.
They conduct assessments, codevelop action plans with PLWHA, and coordinate care.
HSNs are trained to provide empathetic support to vulnerable PLWHA. This personal approach alleviates PLWHA’s fears about linking and engaging in care, and offers them an opportunity to learn how to navigate the health system on their own.
They also serve as advocates for clients, acting as a liaison between the patient’s medical providers, case managers, and other clinical staff.
Slide #37: Health System Navigation/Retention in Care Coordination Logic Model
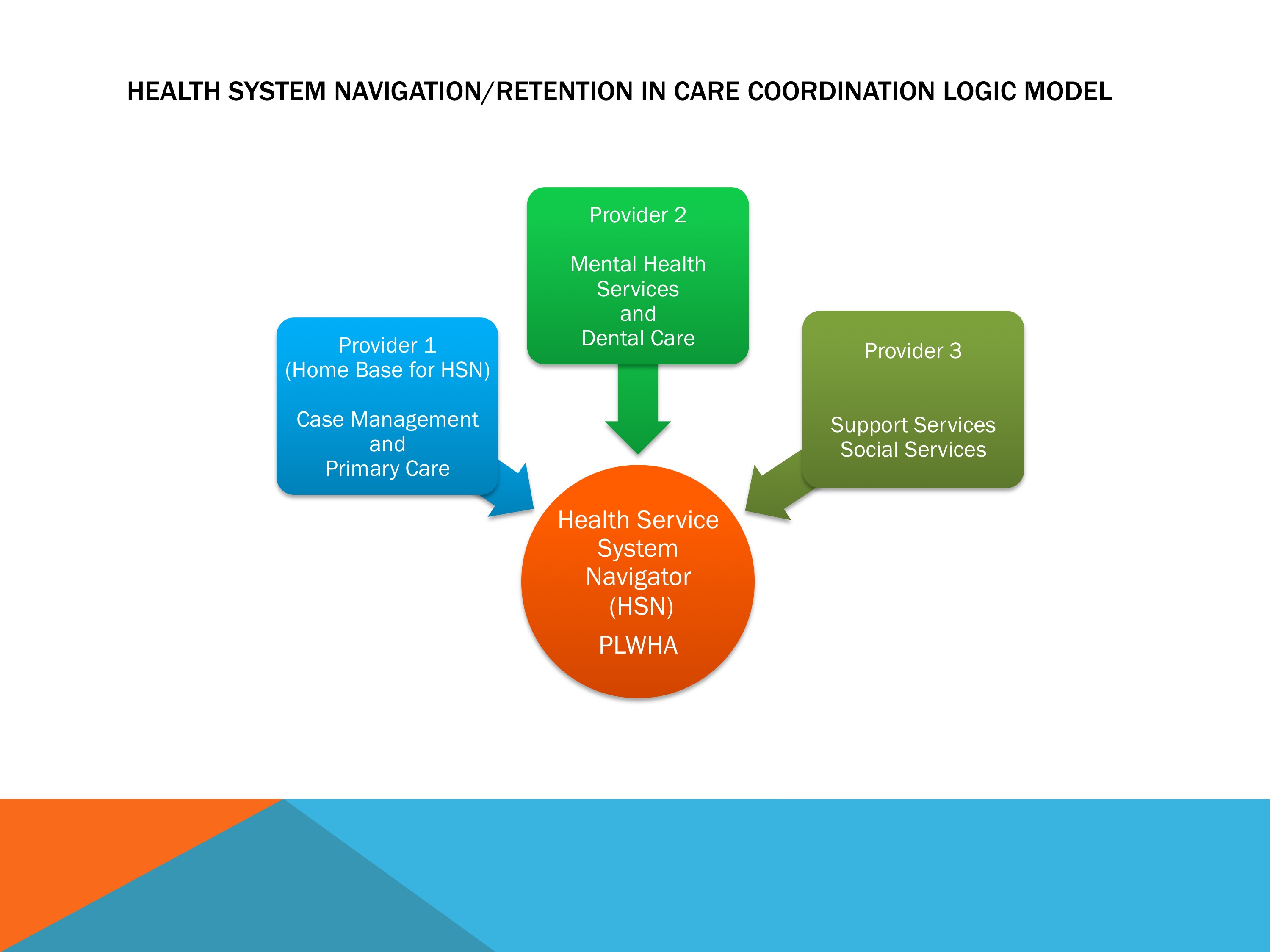
Here we have the HSN/retention in care coordination logic model.
We follow a patient from initial encounter to engagement in care.
HSNs normally follow these steps in linking PLWHA to care:
- The HSN’s clinic or agency partners with one or more organizations.
- Unstable PLWHA are identified at each organization through interviews and other channels.
- Patients identified as unstable in care are assigned an HSN, who conducts assessments designed to identify their care goals.
- HSNs help patients become fully engaged and retained in care, as well as stay treatment-adherent. This is accomplished through intensive clinic contacts that include, but are not limited to:
– Appointment reminder calls.
– Chaperoned visits to medical and support service appointments, court dates, health education classes, and so on.
– Provision or linkage to housing assistance.
– Linkage to or provision of medical case management.
– Additional support to PLWHA who are experiencing challenges with remaining engaged in care. For instance, patients may be offered directly observed therapy, where HSNs and/or other staff help PLWHA take their medications, ensuring ART adherence. - These steps help improve the health and well-being of PLWHA.
Slide #38: Health System Navigation/Retention in Care Coordination Logic Model
Some hallmarks of HSNs:
- HSN services include time-limited intensive case management. After a set amount of time, HSNs generally follow up with PLWHA at 6 and then 18 months, depending on the protocol of their clinic.
- HSNs often are employed by a single clinic or agency, but work with a network of partnering providers to engage PLWHA into care.
- In this manner, PLWHA are provided a virtual medical home, where core medical and ancillary care services are coordinated across different providers, often in close proximity to one another.
- While highly successful with vulnerable PLWHA, this model can cause staff burnout.
- Establishing memoranda of understanding (MOUs) can help clarify provider relationships and expectations.
The Facilitator may want to ask an HSN to come speak to participants if there are none on staff.
Please be sure to tell HSNs in advance not to use their patient’s real names or any other identifying information. You may want to ask HSNs the following questions for them to address in their talk:
- What does it take to be an HSN?
- What type of training did you receive to become an HSN?
- Would you suggest additional training?
- Is there a personality type that works best in this role? Should HSNs be patient? Tough?
- Does it help to have HSNs mirror the PLWHA they serve? That is, should they be peers or near-peers?
- Do you think the clinic has the capacity to train current, or recruit new, employees to become HSNs?
- How did you identify PLWHA? Did you interview them or were they assigned to you?
- Did your work help create a virtual “medical home” for the PLWHA you served? What were the challenges and benefits of working with different agencies to coordinate care? Can you provide some examples from your current and/or previous work?
- With what types of agencies did you (do you) work? Were these official partnerships, such as those brokered through an official MOU or tacit agreement? How did you maintain communication?
- How many PLWHA did you serve? Did you feel your caseload was heavy? Did you ever feel you might burn out? What about the HSNs with whom you worked? How do you try to avoid burnout?
- Intensive guidance is supposed to be provided to PLWHA during a set time period. Did you find that PLWHA became fully engaged—and ultimately retained—in care? Were they able to take over their own primary care, support, and social services routine after that time?
- The literature says that HSNs generally follow up at regular time intervals, depending on the needs of the clients and the resources of the home agency and its partners. How often did you follow up with your patients?
- Was this type of enhanced support helpful to PLWHA currently not in care or unstable in care? Both?
- What are the life and health circumstances of PLWHA who generally need enhanced support from an HSN?
Lead the group evaluation discussion concerning whether this model of care will work for the clinic. Have participants refer to the Model of Care Evaluation Handout from Module 3.
Tape several pieces of paper with the model of care’s title on each.
Slide #39: Group Module Evaluation
Read each question and then write down everyone’s thoughts, questions, suggestions, etc. on paper.
- Can this model of care be readily integrated within the clinic’s current operations and help it reach targeted populations of PLWHA?
- Does the clinic already use this model of care, perhaps in a slightly different form?
- Can the clinic satisfy all requirements for this model of care?
- What funding streams, staffing, materials, and other resources are necessary to implement this model of care? Does the clinic have access to these? If not, how will they access them?
- How will buy-in be secured within the clinic?
- Will the implemented model of care be promoted to potential patients? If so, how? Online through social networks? Word of mouth?
- Does this model of care help the clinic identify and engage targeted PLWHA populations into care?
If more than 10 people are present, the Facilitator may split participants into two or three groups to discuss the following questions and write their thoughts on paper. After a few minutes, the Facilitator should reconvene participants. Representatives from each group will explain their colleagues’ thoughts.
Save the paper/notes from this and previous modules for reference in future sessions.