In response to clinic operation curtailments during coronavirus disease (COVID-19) lockdowns, telehealth services have reportedly expanded across the nation, with subsequent federal support, helping to help maintain connections between patients and care providers.
Expanded telehealth, however, is just the tip of the innovation iceberg. This blog describes how various entities that provide services funded by HRSA HIV/AIDS Bureau’s (HAB) Ryan White HIV/AIDS Program (RWHAP) have adapted operations in response. Featured are programs in California, Illinois, Indiana, New Jersey, and Washington State. Agencies have crafted and modified processes to conduct eligibility assessments, fill prescriptions, keep insurance coverage in place, and community-wide efforts to provide help with varied needs: groceries and rent to the newly unemployed. Chicago and Los Angeles are just examples of much more. Staff are also keeping in contact with each other as they undertake what amounts to telework on steroids, features of which may remain the norm as the world starts to reopen and rebound.
Adjusting Policies and Procedures (Eligibility, Forms, Prescriptions, Insurance) | Communicating Differently | Food and Rent
Adjusting Policies and Procedures

Two RWHAP Part B recipients, Indiana and Illinois, represent how many states have quickly created new procedures for RWHAP subrecipients to adjust to COVID-19. Their efforts meet the flexibility standard outlined in HRSA HAB's COVID-19 Frequently Asked Questions. "We had expected we would be moving toward adjustments during the emerging pandemic so our program was preparing," said Jeffrey Maras, Illinois Ryan White Part B Administrator, referencing the state's issuance of its stay-at-home order on March 17. The Illinois RWHAP Part B program issued many of its adjustments in a detailed Policy Clarification Notice with guidance topics like use of grant funds and client eligibility assessments. Indiana also made similar adjustments, like procedures for work-at-home staff on handling client interactions.
Eligibility and Recertification
Stay-at-home orders put an end to most face-to-face appointments and putting pen to ink in filing paperwork. The Indiana Department of Health created procedures to handle online processing of client applications and eligibility determinations and redeterminations. Attestations, where clients affirm they meet conditions of eligibility, can be verified by case managers, who are allowed to sign forms for clients and make a special COVID-19 notation in the e-file.
Illinois also developed an attestation letter (in English and Spanish) that could be signed by a case manager to verify insurance, income, and residency. If nothing is changed, the case manager can attest to that and sign on behalf of clients. "This precluded major overhauls of our data system," said Maras, adding "we didn’t want clients and staff to have to be forced to meet face to face." (Illinois even created a one-page instruction sheet on how to take a photo of their forms and edit the photo to sign it.)
Attestations are uploaded by case managers or other team members in the state's secure online portal, which clients can also access. "Clients have the ability to monitor, 24/7, the status of their eligibility processing" said Maras. "We encourage clients to set up user accounts through our user system, where they can receive texts and email messages from the state health department on the status of eligibility," providing "real-time updates."
Waivers
Illinois' Ryan White has a "four pillars" test for eligibility, according to Maras: residency, HIV status, third-party payer, and documented viral load results. The state can grant waivers in certain situations, such as when a client is unable to get updated lab results during the six-month recertification period. Illinois initially granted 30-day waivers but extended that to 60 days "as we knew the stay at home was going to be longer than initially anticipated," adding, "this was probably one of the smartest actions we implemented," said Maras.
Keeping track of waivers is critical. There is a comment box in Illinois' online system to document when "a waiver of a pillar of eligibility was allowable, as necessary to accommodate COVID-19 stay at home." However, Illinois also saw a potential problem with waivers in compressing too many future recertifications into one or more single months. Said Maras, "our staff could not handle this quantity of recertifications. We [thus] recoded clients who were reassigned by COVID or regular recertifications" to help keep clients in their regular recertification months.
Filling Prescriptions
Indiana's AIDS Drug Assistance Program (ADAP) now allows 90-day prescription refills for a limited time instead of the prior 30-day refill schedule. Illinois considered a similar change but first contacted their state pharmacy dispenser and wholesale pharmacy. Illinois' drug wholesaler said such an extension would disrupt the drug supply pipeline. Instead, Illinois only does advance refills in emergency cases, such as for several clients who were out of state when informed about their COVID-19 diagnosis and were thus unable to travel back home. Illinois has shipped their medications to them. Illinois also implemented their “disaster relief flag” for out-of-state RWHAP clients who got quarantined while in Illinois. The state verified their ADAP enrollment in their home states--South Carolina and Georgia so far--and then dispensed needed medications to these clients.
Keeping Insurance on Track
Illinois, like many states, pays insurance premiums for certain clients whose coverage is paid by RWHAP Part B. The state processes premium payments via a third-party contractor. "A large number of our clients work in hard-hit service industries," said Maras. The state knew that these newly unemployed individuals would face a months-long delay if the state quickly moved to have them apply for coverage under expanded Medicaid coverage per the Affordable Care Act. Thus, the contractor was told to not switch clients during this time period so as not to disrupt coverage.
Communicating Differently
Because of COVID-19, virtual staff meetings are now routine. Indiana's state health department has regular one-hour sessions to keep staff up-to-date and review projects and tasks. Illinois also has daily briefings with those employees working remotely to ensure guidance continuity and support.
In their meetings, Indiana asks sites to share their best practices. One agency, Indiana University Health, highlighted their daily 15-minute morning check-in to share information and expectations for the day. The agency also described how one person comes into the main office and "prepares immediate client needs (medications, Ensure, food, toiletries, etc.) each day and leaves them in the (locked) entry to our building for staff to pick up without coming in." Another task is scanning the email inbox daily and turfing that information to the right staff person. Said the staffer: "It’s weird, but it’s working pretty well."
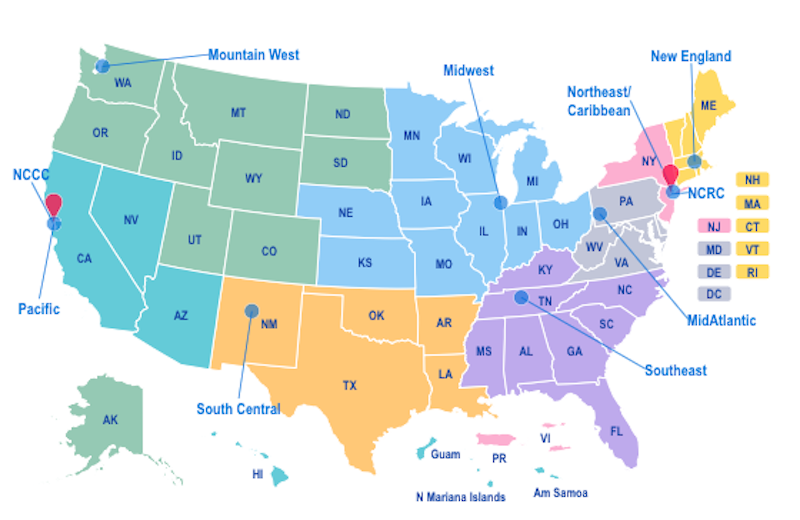
Similar remote collaboration happens at the Northeast/Caribbean AIDS Education and Training Center (NECA). NECA holds regular virtual meetings, including a “drop in” meeting every Thursday morning to provide an open forum for staff discussions across regional partners. These often run to an hour as the scheduled 30 minutes is not enough.
Jefferson Health, the South Jersey local partner of NECA has created a series of COVID-focused educational sessions for local providers that cover these topics:
- COVID-19 Update for Community-Based Organizations and Allied Health Professionals
- COVID-19 and the Intersection with HIV and Behavioral Health
- COVID-19 and the Intersection with HIV and Housing (in partnership with the NJ Housing Collaborative)
- Patient Engagement during COVID Pandemic (with background on coronavirus and information about the agency's response)
NECA also convenes biweekly calls, Just in Time Strategies: Agency-Based Change Best Practice Network. They focus on a change that has been implemented by agencies participating in the New Jersey Behavioral Health HIV Integration Project (BHIP) within their network.
Food and Rent: Helping Fill Basic Needs
Tens of millions of Americans have been laid off within a short time frame. Many of those jobs were at or near minimum wage. The next meal and rent payment was always going to be a challenge. TargetHIV learned about what cities like Los Angeles are doing when responding to a Help Desk question from a recently unemployed gig worker with MediCal coverage and access to medications in search of financial relief. Examples of help in Los Angeles for low-wage workers dealing with COVID-19 hardships include food banks, online food purchasing, a debit card (enrollment closed as the program reached its limit), and much more, like the services outlined in the LA Community Resources Guide - COVID-19. Los Angeles also maintains its HIV Connect portal for HIV services across the county.
TargetHIV was able to pull information together on Los Angeles activities via front-line RWHAP staff, including Tom Donohoe of UCLA, who directs the Los Angeles Area AETC (Pacific Region AETC) and works on other RWHAP projects, including the new TAP-IN project to support jurisdictions funded under the Ending the HIV Epidemic: A Plan for America. Donohoe also tapped into his network, including AltaMed, another RWHAP agency.
In Chicago, the HIV Resource Hub portal for HIV-related services was modified to help individuals apply for one-time emergency rent and utility assistance around COVID-19. We learned about this effort in a recent AIDS Foundation of Chicago's listserv. The HIV Resource Hub was established in February 2020 in the pre-COVID-19 era by AIDS Foundation of Chicago and the Center on Halsted. The Hub's broader purpose is to help link people to HIV care and other services as well as PrEP.