
Search »
Search tips
- Use quotation marks (e.g., "RSR Manual") to search for exact phrases.
- You must be logged in to search for people in the Ryan White/TargetHIV community.
Filters
Content type
Topic Areas
Source
Publication Date
Found 4737 results.
- HIV Care Continuum
The HIV care continuum is a representation of the extent to which individuals living with HIV are diagnosed, engaged in care and benefiting from antiretroviral therapy in terms of full viral suppression (undetectable lab values). The value of the continuum in managing the HIV epidemic is compelling: individuals engaged in care can manage HIV as a chronic condition and simultaneously reduce the risk of transmitting the virus to others.
- Stigma/Legal
HIV-related stigma compromises the well-being of people with the disease. Stigmatized individuals may suffer discrimination that can lead to loss of employment and housing, estrangement from family and society, and increased risk of violence. HIV-related stigma can also drive new HIV infections because it can deter people from getting tested for the disease, make them less likely to acknowledge their risk of infection, and discourage those who are HIV-positive from discussing their HIV status with their partners and families.
- Aging / Older (50+)
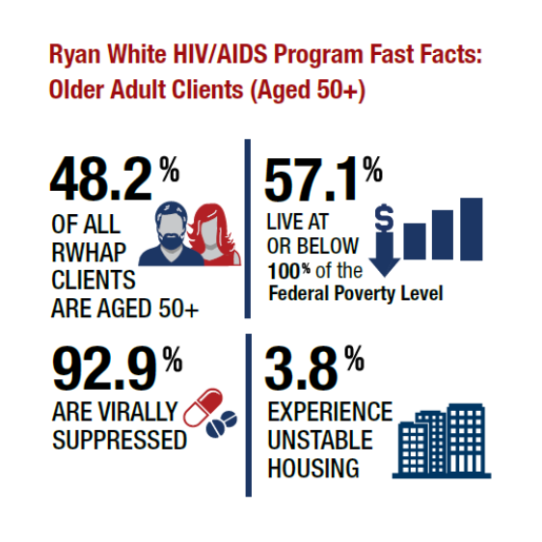
Nearly half of Ryan White HIV/AIDS Program (RWHAP) clients are aged 50 years and older. As with the overall RWHAP population, the majority of older Ryan White clients are from racial and ethnic minority populations and have lower incomes. Their viral suppression rates, across key populations, are slightly above the overall RWHAP rate, with the exception of those with unstable housing. Care for older people can be challenging if they are being treated for multiple conditions as they may need support to manage (and pay for) complicated treatment regimens.
- Performance Measurement
The HRSA HIV/AIDS Bureau's performance measure portfolio is a set of standardized measures aligned with milestones along the HIV care continuum. Ryan White HIV/AIDS Program recipients are encouraged to use them, including the core performance measures, which completed the rigorous National Quality Forum infectious disease endorsement process.
- Completeness
HAB’s RSR data quality goal is for all providers to have at least 90% known values – that is valid data excluding missing or unknown values – for five client-level data elements: health insurance status, housing status, federal poverty level, viral load, and prescribed ART. These data elements are required to both establish Ryan White eligibility and demonstrate critical HIV health outcomes.
- COVID-19 Data Report (CDR)
To support federal requirements to monitor and report on funds distributed under the CARES Act, the HRSA HIV/AIDS Bureau (HAB) created a new data reporting module – the COVID-19 Data Report (CDR) – to collect information on CARES Act funded activities. The CDR will collect monthly, aggregate data on the types of services provided and number of people served for the treatment or prevention of COVID-19 among RWHAP-eligible clients. Completion of the CDR is required for all providers (regardless of whether they are recipients or subrecipients) who receive CARES Act funding.
Access the COVID-19 Data Report.
- Estimating Unmet Need
Update to the Unmet Need framework for Ryan White HIV/AIDS Program (RWHAP) Part A and Part B recipients, by HRSA's HIV/AIDS Bureau. RWHAP Part A and Part B recipients will be required to submit Unmet Need estimates using the updated methodology in FY 2022 as part of their applications. Listed resources are to assist recipients with the successful implementation of the new methodology, which was developed given improvements in the availability and quality of data used to estimate unmet need.
- Methodology for Estimating Unmet Need: Instruction Manual and accompanying materials that focus on various aspects of the unmet need methodology
- The latest Estimating Unmet Need: Required Reporting Templates and Optional Calculation Tables Package
- Go beyond the basics with various webinars and training
- Employment Support for People with HIV
HIV agencies often focus on employment services--for people with HIV as well as their staff. For patients/consumers, employment support is increasingly crucial given the disproportionate impact of HIV on lower income individuals, who are living long and hopefully productive lives given the effectiveness of HIV treatment and care. Support may include, for example, job training, hiring of peers to work with clients (e.g., peer educators, peer navigators), and support for individuals transitioning from correctional facilities.
See Program Management and the AETC NCRC Library for resources on workforce support on conducting services in new and innovative ways (e.g., via practice transformation training).
- Service Models
This website is in the process of consolidating HIV care delivery service models within a unified database. In the interim, see the following service models, HIV Care Innovations: Replication Resources and Best Practices Compilation.
- Telehealth
Telehealth is the provision of medical services at a distance via technology. Telehealth has been around for several decades and includes a wide range of methods (e.g., phone, video conferencing, text messaging, mobile apps). Telehealth is used for clinician/client appointments as well as clinician-to-clinician consultations. Telehealth can help break down challenges like transportation and patient stigma fears over going to an HIV care site.
Learn more at Telehealth.hhs.gov and HRSA Telehealth Programs
- Black/African American
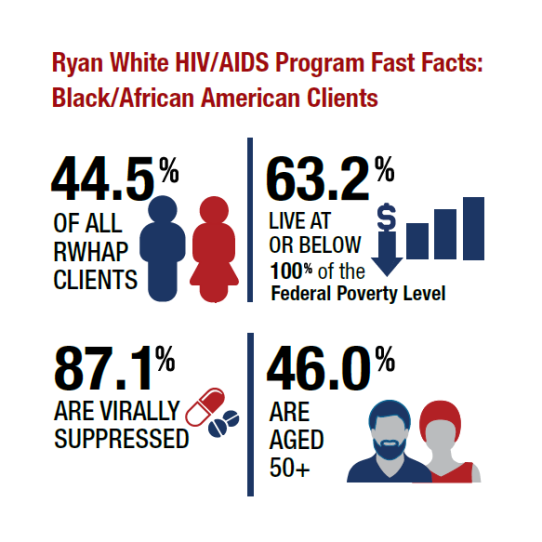
Nearly half of those getting care from HRSA’s Ryan White HIV/AIDS Program (RWHAP) are black/African American. Viral suppression rates are comparable to the overall RWHAP client population, but disparities remain. HIV care programs and technical assistance and training focus on overcoming such challenges as limited access to health services, stigma due to sexual orientation, and housing.
- Collaboration
People with HIV often have a range of medical and support needs that may be met more efficiently when agencies work together. Collaboration takes various forms, like referral arrangements, planning (e.g., sharing of data, participation in planning), common fiscal/grants management processes, single intake/eligibility systems, and sharing/adoption of best practices in HIV service delivery.
- Data Utilization
Data can be used to educate agency leaders and other decision-makers in order to lead efforts toward changes and enhancement of HIV care and public health approaches to ending the HIV epidemic and curing hepatitis C. Data utilization can be applied in the design of agency services, community planning, integration of data systems, and identification of cluster outbreaks.
- Disparities
Quality improvement activities seek to improve care delivery. Efforts that focus on disparities are designed to identify disparities faced by specific subpopulations, most often those that are attributable to social determinants of health, in order to improve their health outcomes.
Access create+equity Collaborative and end+disparities ECHO Collaborative tools.
- Emerging and Innovative Models
HRSA’s HIV/AIDS Bureau has adopted a broad strategy for identifying HIV service delivery models. At one end of the spectrum are relatively flexible criteria for identifying emerging and innovative models, based on “real world” efficacy. At the other end of the spectrum are more rigorous evidence-informed standards.
- Integrated Care
Some care delivery models are designed to address multiple care needs in addition to HIV. Conditions include substance abuse, hepatitis, attention to HIV prevention and care, and services for specific populations (e.g., youth, women). Integrated care can be achieved by, for example, a mix of staff and collaboration across service departments.
- Interdisciplinary Teams
Involvement of staff from a range of professions is utilized by some HIV care agencies so that varied client issues can be addressed within the context of a single agency’s care team. Disciplines may include not only HIV clinical care but also opioid treatment, population-specific care expertise, and other areas of experience.
- Hispanic/Latino
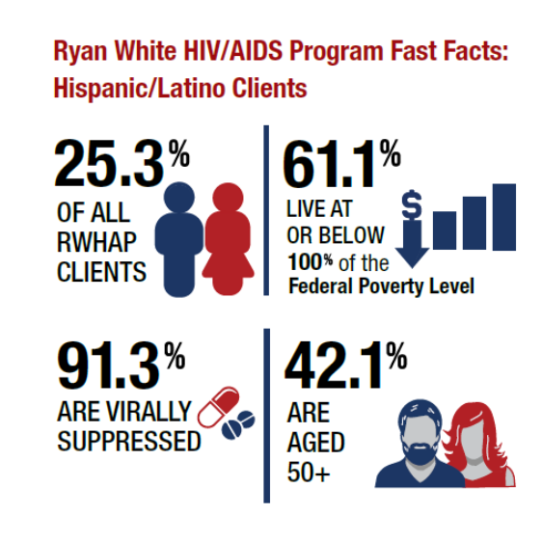
Approximately one-fourth of HRSA Ryan White HIV/AIDS Program (RWHAP) clients are Hispanic/Latino. Viral suppression rates are slightly above the overall RWHAP average, and overall these clients are younger than average. Technical assistance and training resources focus on, for example, linguistic, cultural, and other barriers to health care.
- Leadership
Involvement of people with HIV is a hallmark of HRSA’s Ryan White HIV/AIDS Program (RWHAP). Leadership of people with HIV takes many forms, from meaningful participation in planning, community advisory boards, and positions in agencies are staff.
- People with Disabilities
Ensuring access for persons with HIV who have disabilities can include, for example, physical access to facilities; presentation of content for those with visual and hearing challenges; and delivery of services for those with cognitive barriers.